

Background: Data from the phase 2, single-arm ENESTfreedom study (NCT01784068) have demonstrated the feasibility of treatment-free remission (TFR) following front-line nilotinib (NIL) treatment, with substantial TFR rates being sustained over time among patients (pts) with chronic myeloid leukemia in chronic phase (CML-CP). Results for long-term outcomes after a 5-year follow-up are presented here. The current subanalysis evaluated the efficacy and safety of TFR after upfront treatment with NIL in older (≥65 years [yrs] at study entry) vs younger (<65 yrs) pts.
Methods: Adult pts enrolled in ENESTfreedom had achieved MR4.5 after ≥2 years of front-line treatment with NIL. They then entered a 52-week consolidation (CONS) phase in which they continued treatment with NIL 300 mg twice-daily; pts still in MR4.5 at the end of CONS entered the TFR phase. NIL treatment was re-initiated upon loss of major molecular response (MMR). Rates of MMR and MR4.5, as well as safety, were evaluated according to age group (<65 yrs vs ≥65 yrs). Molecular response data are reported for pts who entered the TFR phase (n=190), while safety data are reported for pts in each study phase (CONS, TFR or re-initiation).
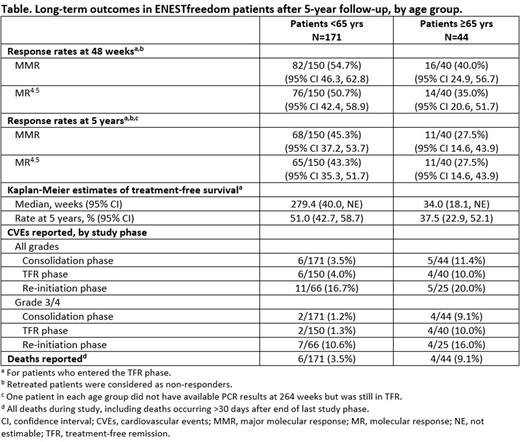
Results: The total number of pts analyzed was 215, of which 171 were <65 yrs and 44 were ≥65 yrs (age range at study entry 21-86 yrs). Of the 190 pts who entered TFR, 40 were ≥65 yrs. Compared with pts <65 yrs, higher proportions of pts ≥65 yrs had arterial hypertension (60.0% vs 34.0%), diabetes mellitus (10.0% vs 3.3%) and hypercholesterolemia (22.5% vs 14.7%) at baseline. The median time from first achieving MR4.5 until TFR entry was 30.7 months (range 12.3, 83.0) for pts <65 yrs and 27.2 months (range 12.3, 43.9) for pts ≥65 yrs. Median duration of NIL treatment until TFR entry was 43.5 months (range 32.9, 88.7) for pts <65 yrs and 43.3 months (range 36.9, 49.2) for pts ≥65 yrs. After 48 weeks in TFR, 82/150 (54.7%) and 76/150 (50.7%) of pts <65 yrs remained in MMR and MR4.5, respectively, compared with 16/40 (40.0%) and 14/40 (35.0%) for pts ≥65 yrs. Five years after the start of the TFR phase, 69/150 (46.0%) pts <65 yrs were still in TFR, compared with 12/40 (30.0%) pts ≥65 yrs. The Kaplan-Meier estimate rate of treatment-free survival at 5 yrs was 51.0% (95% CI 42.7, 58.7) for pts <65 yrs and 37.5% (95% CI 22.9, 52.1) for pts ≥65 yrs. Incidence of all-grade adverse events (AEs) was comparable between age groups (<65 yrs vs ≥65 yrs) across the CONS (84.2% vs 86.4%), TFR (80.7% vs 65%) and re-initiation phases (95.5% vs 96%), but higher incidence of grade 3/4 events was observed for pts ≥65 yrs in the CONS phase (31.8% vs 11.7% in pts <65 yrs) and the re-initiation phase (76.0% vs 42.4% for pts <65 yrs). The proportion of pts with all-grade and grade 3/4 cardiovascular events (CVEs) was increased in pts ≥65 yrs vs pts <65 yrs across all study phases. The highest incidence of CVEs was observed for all pts in the re-initiation phase, where the proportions of pts experiencing all-grade CVEs did not differ substantially among age groups (20.0% for pts ≥65 yrs vs 16.7% for pts <65 yrs). Lower proportions of pts ≥65 yrs experienced increases in blood cholesterol in the CONS phase (2.3% vs 5.8% in pts <65 yrs) and in the re-initiation phase (12.0% vs 21.2% in pts <65 yrs), while similar proportions of pts in both groups reported increased blood glucose levels. Discontinuation from study due to AEs occurred in 4.5% of pts ≥65 yrs (vs 1.8% of pts <65 yrs) in the CONS phase and 28.0% of pts in the treatment re-initiation phase (vs 13.6% of pts <65 yrs); no discontinuation due to AEs was reported in the TFR phase. Four deaths were reported during the study among the 44 pts ≥65 yrs, compared with 6 among the 171 pts <65 yrs. None of the deaths reported were CML-related. Conclusions: Lower proportions of pts ≥65 yrs who achieved MR4.5 following upfront treatment with NIL for ≥2 yrs remained in MMR/MR4.5 after NIL discontinuation compared with pts <65 yrs. The frequency of CVEs was increased in older pts, as expected due to the higher proportion of pts with pre-existing cardiovascular risk factors, such as arterial hypertension, hypercholesterolemia and diabetes mellitus at study entry. Results should be interpreted with caution due to the small sample size for older patient subgroups. Further studies are required to establish whether NIL discontinuation is associated with a longer-term reduction in CVEs. These data suggest that TFR is a feasible management choice for older pts with CML-CP.
García Gutiérrez:Novartis Pharma AG: Consultancy, Honoraria, Research Funding; Bristol-Myers Squibb: Consultancy, Honoraria, Research Funding; Pfizer: Consultancy, Honoraria, Research Funding; Incyte: Consultancy, Honoraria, Research Funding. Radich:Jazz: Consultancy; Amgen: Consultancy; Bristol-Myers Squibb: Consultancy; Novartis Pharmaceuticals Corporation: Consultancy, Research Funding. Hochhaus:MSD: Research Funding; Bristol-Myers Squibb: Honoraria, Research Funding; Incyte: Honoraria, Research Funding; Novartis: Honoraria, Research Funding; Pfizer: Honoraria, Research Funding; Takeda: Honoraria. Saglio:Roche: Research Funding; Ariad: Research Funding; Incyte: Research Funding; Novartis: Research Funding; Bristol-Myers Squibb: Research Funding; Pfizer: Research Funding. Conneally:Novartis: Consultancy, Research Funding; Bristol-Myers Squibb: Honoraria; Pfizer: Honoraria; Gilead: Honoraria. le Coutre:Incyte: Honoraria; Pfizer: Honoraria; Novartis: Honoraria. Gattermann:Novartis: Honoraria, Research Funding. Saussele:Pfizer: Honoraria; Incyte: Honoraria, Research Funding; Bristol-Myers Squibb: Honoraria, Research Funding; Novartis: Honoraria, Research Funding. Giles:Actuate Therapeutics Inc: Consultancy; Pfizer: Research Funding; Novartis: Consultancy, Research Funding. Aimone:Novartis: Current Employment. Li:Novartis: Current Employment. Titorenko:Novartis: Current Employment. Ross:Celgene: Research Funding; Bristol-Myers Squibb: Honoraria; Novartis: Honoraria, Other: Participated in advisory board meetings, Research Funding.

This feature is available to Subscribers Only
Sign In or Create an Account Close Modal